The following outlines are portions from two presentations given for the course 6710 Counseling in Theological Perspective: Faith & Practice taught by Dr. Rev. Stephen Greggo at Trinity Evangelical Divinity School, Deerfield, Illinois, October and November 2014.
The two presentations (part 1 and part 2) addressed a case study of a specific (fictional) individual. My group was selected to address matters related to the use of psychotropic medication and discipline.
The first presentation raised concerns. For example, some of the more theologically oriented concerns regarding the use of medication included the following:
- Not taking responsibility for one’s actions (sin).
- In the use of medication, have we mislabeled sin as illness? Are we treating sin as non-sin?
- By treating an issue as illness, do we eliminate the Christian claim of human responsibility?
- Sanctification – Does medication conflict with the Christian view of change?
- What is genuine, God-honoring change from a Christian perspective (sanctification)? And how is that sort of changed accomplished?
- Is change resulting from medication that form of change, an expression of sanctification? Or should we distinguish the two?
- And if distinguished, how should a Christian view change resulting from medication, since it is not necessarily the change of sanctification? Is to be avoided, seen as good but yet superficial, etc. What?
- Is medication adequate for treating mental illness and acting out behaviors?
- Just because a person is taking medication at one therapeutic level (effective for treating the diagnosed problem) does not mean that all parts of the presenting problem are being adequately addressed.
- One must consider the bio-psycho-social-spiritual dimensions of concern. Medication addresses the biological.
The second presentation provided answers and conclusions. The following is my outline presentation for this second presentation in which I present Biblical and theological foundations for our case study.
Anthropological foundations
- Holistic anthropology – Humans are psychosomatic unions—both physiological and spiritual beings – Deut 6:5 (cf. Mt 22:37; Lk 10:27); 2 Cor 4:16; 1 Thes 5:23.
- The spiritual and physiological effects of sin: Sinfulness and sin have spiritual (Gen 8:21; Jn 8:34; Rom 1:21; 3:10-18; etc.) as well as psychological effects (Gen 2:17; 3:19; Rom 5:12; 6:12-13, 23; 1 Cor 15:21; Js 1:15; etc.).
Conclusions: These realities legitimize the concern for addressing matters physiologically (e.g., with psychotropic medication) rather than just “spiritually.
But it also warns us of the danger of addressing matters as purely physiological, as if physiological matters are non-spiritual matters and psychotropic interventions are sufficient therapy.
Question: Is either medication or discipline adequate in itself for treating mental illness and acting out behaviors?
A dichotomy between spiritual and physical is too simplistic and does not correspond to human nature. We need to attend to both.
“We exist as body-spirit creatures. We are simultaneously body and soul. There’s never a time we’re not spiritually engaged. And there’s never a time we are not bodily engaged. This means that attention to both physical and spiritual aspects of our personhood is mandatory in ministry.” (Emlet, Prozac, 16, emphasis added).
“We should not approach human problems with the false dichotomy: Is this problem spiritual or physical? Rather, we should consider how the physical is affecting the spiritual, and vice versa. Thinking in this vein prevents the counselor from concluding that a problem is physical while ignoring spiritual influences, and vice versa” (Jeremy Pierre, 2012).
Medicine
Initial questions:
- Human responsibility and sin? Does medication conflict with responsibility and sin,mislabeling sin as illness andeliminate responsibility?
- The relationship between sin and physiological problems:
- Illness (presumably including mental illness) can be caused by or linked to personal conscious sin[1] and God’s discipline[2] or punishment of it.[3]
- However, not all physiological effects of sin/sinfulness are a result of personal conscious sin.[4] There is not an inevitable link between sin and sickness.
John 9:1-3 (ESV) – “As he passed by, he saw a man blind from birth. 2 And his disciples asked him, “Rabbi, who sinned, this man or his parents, that he was born blind?” 3 Jesus answered, “It was not that this man sinned, or his parents, but that the works of God might be displayed in him.”
- Continuum:
- The relationship between sin and physiological problems:
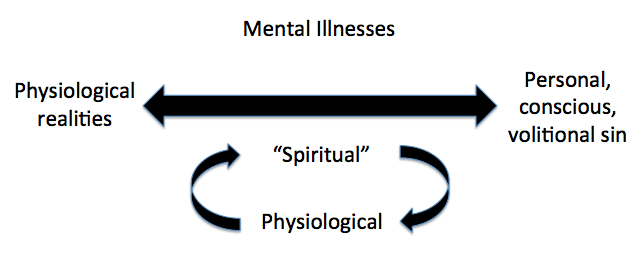
There is never a time when human actions or conditions are purely spiritual or physiological. But for heuristic purposes we can distinguish between personal, conscious, volitions sins (e.g., lying), for which one is responsible, and conditions that are not (necessarily) related to such acts of sin but are a part of the general consequences and effects of sin (e.g., cancer, a broken leg), for which one is not personally responsible.
Between these two poles is a continuum of conditions in which physiological realities are present along with a level of personal responsibility. Many incidences of mental illnesses would seem to fall somewhere within this continuum (variation), having physiologically elements and degrees of personal responsibility.
That mental illness involves both physiological as well as “spiritual” components, and that these components are interconnected and mutually influence one another, fits a holistic Christian view of humans.
Therefore, we are dealing with an issue where there are physiological elements affecting the client but also elements of personal responsibility and sin that must be maintained in treatment. It would be reductionistic to explain the situation in purely spiritual or physical terms. Thus, neither medication or discipline is to be the totality of treatment offered.
- Sanctification? Is the change resulting from medication an expression of sanctification, that change which is God-honoring in the ultimate sense?
No. We should distinguish sanctification—redemptive change accomplished by union with Christ through the work of the Holy Spirit—with change that is common to saved and unsaved alike. We should distinguish deep root change, springing from a heart of faith, from symptom relief.
“Works done by unregenerate men, although for the matter of them they may be things which God commands; and of good use both to themselves and others: yet, because they proceed not from an heart purified by faith; nor are done in a right manner, according to the Word; nor to a right end, the glory of God, they are therefore sinful, and cannot please God, or make a man meet to receive grace from God: and yet, their neglect of them is more sinful and displeasing unto God.” Westminster Confession of Faith, 16.7.
However, this doesn’t mean change resulting from medication is not good (as we will see below) – Symptom relief is good in and of itself even if it is not the ultimate good people need,[5] i.e., Christ-centered, redemptive, spiritual restoration.
Nor is this change necessarily mutually exclusive from sanctification.
“Can taking a medication actually assist in sanctification? Yes, in the same way that adequate sleep can assist in sanctification! It’s not that you can buy holiness in a pill, but using medication in certain situations may help set bodily conditions that allow for a greater spiritual flourishing.” (Emlet, Prozac, 19)
Concerns to uphold: Although we recognize that…
- God uses suffering for good.[6]
- The Bible warns against undue reliance on medical treatment in opposition to trusting in God.[7]
- Relief of symptoms is a potential mitigation of motivation for spiritual growth (Michael R. Emlet, 2008, p. 17)
…We also recognize the following as equally true.
The validity and goodness of mental health care through medication:
- Medicine in scripture: Scripture speaks non-judgmentally and positively of the use of medication and physicians.[8]
- The creation mandate: The creation mandate of exercising dominion over the entire creation in ways that express God’s reign (Gen 1:26; Ps 8) implies mitigating the effects of sin by bringing order to the realm of mental illness. And that includes, at least potentially, the use of psychiatric medication. (Jeremy Pierre, 2012)
- Incarnation (and resurrection): “God’s incarnation … means that God’s redemptive care is not limited to ephemeral, spiritual realities; God loves materiality, and longs to see it healed wherever it may be broken” (McMinn & Campbell, 2007, p. 47).
- Kingdom agenda: “It is a kingdom agenda to relieve our suffering…. When the kingdom comes in Jesus Christ, you see God’s heart with regard to suffering… [e.g., Jesus’ healing ministry]. It is God’s design to relieve the suffering that arose as a result of the fall” (Michael R. Emlet, 2008, p. 16).
- Common grace: We recognize medical treatment and the relief of suffering as an expression of God’s common grace (Lambert, 2014). It is not special grace (sanctification); but it is still legitimate grace.
Notes
[1] Ps 119:67; Jn 5:14; Js 5:13-16.
[2] Prov 3:11-12; 1 Cor 11:27-32; Heb 12:3-11.
[3] Ex 4:24; Num 12:10; 1 Sam 5:6; 2 Sam 24:15-17; 2 Kgs 5:25-27; 19:35; 2 Chron 13:20; 26:16–21; Jer 24:10; 32:24; Ezek 14:21; Acts 5:5, 10; 12:21–23; 13:11.
[4] Jn 9:1-3 (cf. Ex 20:5); cf. Job; Lk 13:1-5.
[5] Illustration – Mission work that focuses on temporal needs, e.g., hospitals, orphanages, shelters, etc. These things are no doubt good, even if they are not the ultimate good people need.
[6] 2 Kgs 20:1-7; Phil 3:10- 11; Rom 8:17; 2 Cor 4; 2 Cor 1:8-9; 1 Pet 4:12- 13; Js 1:2-4.
McMinn and Campbell offers a response to those who would object that “we should not rush to remove symptoms of psychological pain that might ultimately lead a person to search for God” and “a much deeper spiritual healing.” He states, “There are several problems with this sort of logic. First, it we apply this reasoning consistently, it means that all pain should be viewed as God-given and should not be relived through human effort. … Second, if some pain ought to be relieved by human intervention and others ought not to be relieved, who determines what sort of pain is in which category? … A third problem is that the entire premise may be false. [For example] Do we really know that God is more likely to reach a depressed person than one who is not depressed?” (McMinn & Campbell, 2007, pp. 124–125).
[7] 2 Chron 16:12; Cf. Deut 8:10-14; Judg 2:10-12.
Noteworthy are D. H. Trapnell’s comments on 2 Chron 16:12: “But these may have been pagan, magically minded and worthless, and not really deserving the name of physician” [1996, p. 452]).
[8] Gen 30:14-16; Ex 15:26; Deut 28:27; 2 Sam 4:4; Job 13:4; Prov 17:22; 31:6; Isa 1:6; 38:21; Je. 8:22; 46:11; 51:8; Ezek 30:21; Mt 5:26; Lk 4:23; 5:31; 8:43; 10:34; Col 4:14; 1 Tim 5:23.
Bibliography
E. Ray Clendenen, & York Hershael W. (2003). Discipline. In Chad Brand et al. (Ed.), Holman Illustrated Bible Dictionary (pp. 426–427). Nashville, TN: Holman Bible Publishers.
Garrett, D. A. (1993). Proverbs, Ecclesiastes, Song of Songs (Vol. 14). Nashville, TN: Broadman & Holman Publishers.
Heath Lambert. (2014, Setember). How Can Christians Tell the Difference Between a Spiritual Issue and a Physical One? Retrieved November 1, 2014, from http://www.biblicalcounseling.com/blog/how-can-christians-tell-the-difference-between-a-spiritual-issue-and-a-phys
Holladay, W. L. (1971). A Concise Hebrew and Aramaic Lexicon of the Old Testament, Based Upon the Lexical Work of Ludwig Koehler and Walter Baumgartner. Grand Rapids, MI: Eerdmans.
Jeremy Pierre. (2012, September 24). Psychiatric Medication and the Image of God. Retrieved November 1, 2014, from http://www.thegospelcoalition.org/article/psychiatric-medicationand-the-image-of-god
Keil, Carl Friedrich; Delitzsch, F. (1996). Commentary on the Old Testament (Vol. 6). Peabody, MA: Hendrickson.
Kellemen, B. (2014, June 17). Sufficiency of Scripture and Psychotropic Medication. Retrieved November 1, 2014, from http://biblicalcounselingcoalition.org/blogs/2014/06/17/sufficiency-of-scripture-and-psychotropic-medication/
Michael R. Emlet. (2008). Listening to Prozac . . . and to the Scriptures: A Primer on Psychoactive Medications. The Journal of Biblical Counseling, 26(1), 11–22.
O’Brien, P. T. (1999). The Letter to the Ephesians. Grand Rapids, MI: W.B. Eerdmans Publishing Co.
Welch, E. T. (1998). Blame It on the Brain: Distinguishing Chemical Imbalances, Brain Disorders, and Disobedience. Phillipsburg, NJ: P & R Publishing.
Discover more from Kirk E. Miller
Subscribe to get the latest posts sent to your email.
